Self-acclaimed life coach, Solomon Buchi has advised women not to marry men who cannot protect their family.
He insisted that men who cannot call out and rebuke their parents should be avoided.
Buchi argued that the protective nature of men should not only be in their physical look but also in their ability to be stubborn and firm even towards their own family members.
He opined that men should always be men and protect their family from outsiders.
Speaking via social media, he wrote, “Don’t marry a man who cannot call out and rebuke his parents. The protective nature of men isn’t just in bigger toned muscles but in their ability to be firm, stubborn and bold even to their family. It’s easy to find a man who can protect you from outsiders; please find a man who won’t be scared to protect you from his family if need be. Men ought to be men.”
Why Is The Nigerian Government A Puppet To Bobrisky? – Solomon Buchi
Meanwhile, Buchi has questioned why the Nigerian Government is silent over the attitude of controversial crossdresser, Idris Okunneye, popularly known as Bobrisky.
Naija News reports that this comes amidst the controversy trailing the ‘Best-Dressed’ female award given to Bobrisky at the ‘Ajakaju’ movie premiere over the weekend.
In a post via X, Buchi said Bobrisky might have friends in the Nigerian police force, judiciary, and political space due to his confidence in speaking publicly and doing certain things without being punished.
He added that Bobrisky would have been arrested and prosecuted long ago if he had been a poor man or probably did not have a political godfather in Nigeria.
The post read, “Bobrisky must have friends in high places in Nigeria. Probably in the police, judiciary and random politicians, because his confidence to say and do certain things publicly shows that he’s got political assurance.
“Who is Bobrisky’s political godfather in Nigeria? Why is the Nigerian government a puppet to Bobrisky?
“If Bobrisky were a poor man, shim would have been prosecuted a long time ago. Who’s covering Bobrisky?”
Tears welled, then passionately flowed from Amplify Africa co-founder/CEO Dami Kujembola’s eyes as he looked out at the 400 people clad in traditional African garb at Los Angeles’ Majestic during last year’s Afro Ball Gala, a formal, fashion-forward event that his media and entertainment brand hosts every year to celebrate African individuals excelling in their respective fields. While wearing his Nigerian native in its regal purple glory, Kujembola buried his face in Amplify Africa co-founder/COO Timi Adeyeba’s chest and later marveled at the work of two boys from Lagos, Nigeria who have made it their mission to magnify African culture and unite the global Black diaspora.
“We were just so emotional, hugging each other,” Adeyeba reflects now while discussing the video Kujembola posted “to debunk the myth that Black men shouldn’t cry.” “To see something that we’ve talked about for a long time come to reality was just surreal. Even talking about it now, I have goosebumps.”
Since 2015, Kujembola and Adeyeba have developed Amplify Africa into an influential U.S.-based African media and entertainment brand “with a goal of educating people about the continent, creating representation for the diaspora and giving the diaspora community a pathway to connect back to the continent,” Kujembola says. Amplify Africa has hosted over 250 events in that time, including Afro Ball Gala; AFRICON, a multi-day conference and celebration of African culture, innovation and entrepreneurship that features panels and immersive experiences; and Afrolituation, which describes itself as the “biggest Afrobeats party in North America.”
And while they’ve worked tirelessly to recognize African excellence in others, Kujembola and Adeyeba have also been given their flowers: Two days after AFRICON 2023 concluded, Los Angeles mayor Karen Bass presented them with certificates of recognition for their “devotion to providing service throughout the greater Los Angeles community while remaining connected to the miraculous continent of Africa.”
Working in entertainment had long been the goal for Kujembola and Adeyeba — but from a much different point of view. The two attended law school together at Babcock University in Nigeria in 2007 and were part of the Law Students Association of Nigeria, with Kujembola as attorney general and Adeyeba as social director. Upon graduating from Nigerian Law School, the two separately decided to move to L.A. to pursue entertainment law, with Kujembola attending USC in 2014 and Adeyeba attending UCLA the following year. “When we moved here, it became clear to us that there was massive ignorance about where we came from,” says Adeyeba. “We would hear a lot of ignorant questions about whether we had electricity [or] whether we knew what languages lions speak. We decided we needed to change that narrative.”
In the mid-2010s, one might hear songs like Afro B’s “Drogba (Joanna)” or Drake’s “One Dance,” featuring Wizkid and Kyla — which mixes Afrobeats with dancehall, U.K. funky and more — at a club in the States. But there was no dedicated space for African immigrants to hear their own music outside of their homes. “Because of our backgrounds in entertainment and entertainment law, we built a lot of relationships on the continent with a lot of artists before moving out here,” Kujembola previously told Billboard while discussing Afrolituation. The two hosted their first party in 2016, when Nigerian rapper Falz the Bahd Guy and late South African rapper AKA were in L.A. for the BET Awards as nominees. Since then, Afrolituation has traveled to nine other U.S. cities (as well as international hot spots like Accra, Ghana and Cairo, Egypt); hosted performances by Kizz Daniel, Maleek Berry, Major Lazer and Major League Djz; and attracted A-list guests like Metro Boomin, Future and Brent Faiyaz.
Through Kujembola and Adeyeba’s connections to Afrobeats artists and their teams, they’ve hosted more curated events and worked on music in various capacities. Amplify Africa hosted the official after parties for Wizkid’s Made in Lagos L.A. tour stop in September 2021 and Burna Boy’s historic headlining concert at the Hollywood Bowl the following month, four years after Amplify Africa (alongside BET) hosted Burna for the first time at the BET International After Party at The Belasco. Amplify Africa has also hosted showcases and concerts for ODUMODUBLVCK and Mr. Eazi; Kujembola and Adeyeba assisted the latter with the promotional release for his Apple Music “Up Next” Artist campaign. They’ve also helped Davido with the marketing of his 2019 “Blow My Mind” collaboration with Chris Brown while hosting the song’s release party “within a day’s notice,” adds Kujembola. And they helped A&R the “Mbilo Mbilo (Remix)” by Eddy Kenzo, featuring Niniola.
“While we were doing that, we started the media page and started posting beautiful images of various parts of Africa and positive news about various things happening on the continent,” adds Adeyeba, who notes Amplify Africa has a monthly global reach of 15 million people across its social media accounts, website and newsletter.
But when it came to the company’s practice of highlighting Africans who are excelling in various industries, Kujembola and Adeyeba didn’t have to look further than the people who were attending their own events. Their Afrolituation parties were also attracting entertainment industry leaders, like Def Jam chairman/CEO Tunji Balogun, who could “help us scale other parts of our company,” Kujembola told Billboard last summer. “We also want [Afrolituation] to feel like a networking environment where people of African descent can come and feel like they’re meeting other quality people that are doing amazing things in their profession. You think about [Afro Ball] Gala or AFRICON. We had over 100 speakers last year, and these are people that we’ve interacted with at some of our parties.” And while Afro Ball celebrates successes, AFRICON is a way “for people to actually sit down and share information, inspire, do business together and really build generational wealth together as a people,” says Adeyeba, who adds that outside of the panels, the conference also has a marketplace full of African-owned businesses. (This year’s AFRICON will take place from Sept. 27-29 at L.A.’s Magic Box at the Reef.)
But the Amplify Africa co-founders wanted their mission of “giving the diaspora community a pathway to connect back to the continent” to become even more of a reality. Kujembola remembers the DNA test craze between 2018 and 2020, when people were trying to discover where their families were really from in hopes of one day visiting their home countries. And while African immigrants make up a core audience for Amplify Africa, African Americans who were forcibly removed from their motherlands due to slavery is another key demographic for the company. This inspired Kujembola and Adeyeba to launch Pathway, a one-stop shop for people to discover their African roots through a DNA test; learn more about the food, music, fashion, language, history and more; book travel to the continent; and explore their motherland through the mobile and web platform, which will become available on Sept. 27.
“The whole narrative of our company is to showcase that reconnection to the continent,” Kujembola says.
SPOTLIGHT:
I knew I was committed to music when “we lost about $30,000 on one of our first shows that we did. This was back in 2017. And we still did another show afterwards. At that time, we didn’t even have that money. It was an investment, and we lost the entire thing. I can never forget that one. That’s actually when I knew I was coming into this for real.” — Adeyeba
The best advice I’ve received is “‘it’s not what you lack that limits you, it’s what you have that you don’t know how to use.’ That has been my approach to a lot of things, even with us starting Amplify Africa. It’s always been, ‘Hey, let’s look to the diaspora. We have what we need to be great.’ And we’ve lived by that since the inception.” — Kujembola
Something most people don’t understand is “how much work and how much strategy it takes to put together successful events. Sometimes, people just come and feel like, ‘Oh yeah, it’s just a party. You’re not working.’ People don’t understand that it’s actually a lot of work, like how much sacrifice we’ve actually had to make to continue what we’re pushing for.” — Adeyeba
Spotlight is a Billboard Pro series that aims to highlight those in the music business making innovative or creative moves, or who are succeeding in behind-the-scenes or under-the-radar roles. For submissions for the series, please contact spotlight@billboard.com.
As Africa’s most populous country, with over 200 million people, Nigeria faces a unique set of healthcare challenges. While recent years have witnessed advancements in areas like telemedicine and specialised care centres, significant challenges persist in achieving universal access to quality care according to the World Health Organisation. Some of the challenges being faced within the sector include limited access to essential services, inadequate infrastructure, and a shortage of skilled professionals. However, amidst these challenges lies a beacon of hope for Nigeria – the potential for collaboration and knowledge sharing to drive transformative change and propel the sector forward.
Currently, underserved communities in Nigeria face obstacles when it comes to basic health and well-being due to limited access to state-of-the-art equipment, technology, and healthcare facilities. These three major limitations have forced medical professionals to rely on older, less precise methods, potentially leading to delayed treatment. Furthermore, the absence of cutting-edge technology has continuously hindered preventative measures and early intervention, which are crucial for managing chronic conditions. This disparity is often compounded by a shortage of healthcare facilities, forcing residents to travel long distances for even basic medical attention, creating a significant barrier to care, especially for those with limited transportation or financial resources.
This shortage is a result of various factors, which include brain drain, inadequate training opportunities, and challenges in retaining skilled personnel. To address this challenge, there is an urgent need for improved training programs, retention strategies, and incentives to attract and retain healthcare talent.
Another major obstacle lies in the fragmented nature of the healthcare system. Public health institutions, private hospitals, and non-profit organisations often operate in silos, with limited communication and coordination. This lack of a unified approach hinders the efficient delivery of services such as crucial data sharing and coordinated disease prevention and management strategies.
However, amidst these challenges lies an opportunity for transformation through collaboration, innovation, and knowledge sharing. By bringing together diverse stakeholders, leveraging technology, and investing in human capital, Nigeria can build a healthcare system that is more equitable, efficient, and resilient, ultimately improving the health and well-being of its people. Medic West Africa has over the years positioned itself as a reputable platform that fosters connections and addresses industry challenges. Hosted annually, Medic West Africa is the largest gathering of healthcare stakeholders in the West African region, offering a collective platform for professionals, policymakers, private sector as well as international organisations to explore the latest technological advancements and participate in engaging conversations to address challenges within the healthcare industry.
Scheduled for 17–19 April 2024 at Landmark Centre, Lagos, the 11th edition of Medic West Africa is set to connect over 6,000 healthcare professionals through various thought-provoking conferences and a bustling exhibition floor. The event will serve as a knowledge-sharing hub by bringing together healthcare professionals through conferences featuring expert-led presentations and discussions, exhibitions showcasing cutting-edge technologies and equipment, and dedicated networking spaces. This comprehensive approach will foster collaboration and knowledge exchange between diverse stakeholders, ultimately propelling advancements in West African healthcare.
In a country with diverse healthcare needs and limited resources, collaboration and knowledge sharing are indispensable. By connecting healthcare professionals, researchers, policymakers, and stakeholders, a vibrant ecosystem for sharing insights, experiences, and best practices will emerge. This exchange will not only help in identifying common challenges but will also facilitate the dissemination of innovative solutions tailored to the Nigerian context. Through collaborative efforts, stakeholders can leverage each other’s expertise to develop and implement evidence-based strategies that address local healthcare challenges. Furthermore, by sharing successes and failures, stakeholders can learn from each other, accelerating the adoption of best practices and mitigating potential pitfalls. Ultimately, these partnerships and knowledge exchanges pave the way for sustainable healthcare initiatives that are responsive to the needs of Nigeria’s diverse population.
As healthcare stakeholders continually strive for solutions to industry challenges, the Medic West Africa Exhibition and Conference remains the most valuable platform for connecting stakeholders, facilitating knowledge exchange, and paving the way for a more collaborative and innovative healthcare ecosystem in Nigeria. The 2024 edition of the conference and exhibition will host 32 exhibiting countries, 180+ exhibitors, 3 insightful conferences, and 4 workshops for healthcare professionals. Medic West Africa will continue to stand as the gateway to access the West African healthcare market.
For more information about the Medic West Africa Exhibition and Conference 2024, please visit www.medicwestafrica.com.
Increasing evidence suggests that quality care prevents a significant number of maternal deaths and disability. High-quality care is also the foundation for improved maternal and neonatal health outcomes. According to the World Health Organisation, despite the fact that more women are giving birth in health facilities than ever before, there has still been no significant increase in maternal and infant the survival rates, which is attributed in part or whole to poor quality care in health facilities.
In Abakpa, Kaduna State, Nigeria, a young mother has just given birth. She described the care she received throughout her labour and delivery at a hospital in Giwa. “Immediately I came to the hospital, I was taken to the labour ward, given a bed, and my BP and everything was checked…My contraction wasn’t much, so I was placed on drip and some treatment. Within a moment, I gave birth. Immediately I gave birth; the baby was placed on my chest for me to start breastfeeding after some minutes…I like the way they attended to me,” she shared.
According to the Lancet Commission on High-Quality Health Systems (2018), a strengthened health system that provides high-quality maternity care might prevent half of all maternal and 1 million newborn deaths each year. For this young mother, her childbirth experience was safe, as a result of the quality of care she received.
The SafeCare Methodology of Quality Improvement Emphasising that quality care is the key to reducing maternal mortality in Nigeria, Pathfinder Nigeria and PharmAccess Foundation collaborated with the Kaduna State Ministry of Health to improve the quality of maternal health care in twenty-five (25) private health facilities through the Saving Mothers, Giving Life (SMGL 2.0) project.
The SMGL 2.0 project, implemented in Kaduna State between 2020 and 2023, sought to improve access to and quality of maternal and newborn health services and strengthen collaboration and partnership between the Kaduna State Ministry of Health and the private health sector. The project also worked with traditional birth attendants to improve women’s health-seeking behaviours, referrals and health insurance enrolment. To strengthen accountability for maternal deaths, strategies utilised included the establishment of the Maternal and Perinatal Death Surveillance and Response and the deployment of an interactive digital health chat solution on WhatsApp (AskNivi) in partnership with Nivi to provide relevant maternal and newborn health information to pregnant women.
In improving quality care in the facilities, the project utilised the SafeCare methodology to strengthen the facility’s capacity to provide Emergency Obstetric and Newborn Care (EmONC) and family planning services.
SafeCare is an internationally accredited methodology based on the WHO quality of care framework developed to improve the quality of care in health care settings, (especially in low- and middle-income countries (LMIC)), by implementing a set of standards. These standards are broken down into achievable and measurable steps to facilitate incremental quality improvement.
The SafeCare standards cover both medical and non-medical aspects of care and are structured around four (4) broad service elements: management, clinical, clinical support and ancillary. These four service elements are further divided into 13 categories. A health facility’s performance is measured against the SafeCare standards, and it is awarded a certificate of improvement based on its performance. There are five (5) levels of quality certifications that a health facility can attain under the SafeCare programme, ranging from level 1 (very modest quality) to level 5 (high quality).
Image credit: SafeCare
In the project’s first year, facilities were assessed using SafeCare digital tools to obtain a baseline of the quality of care delivered in each facility. Based on the assessment, 17 of the 25 health facilities fell under level one while the remaining eight were placed on level two. Automated assessment reports, and quality improvement plans (QIP) were then generated and shared with all 25 facilities.
Image source: SafeCare
Following the assessment, selected staff of each of the 25 health facilities were appointed as Quality Improvement (QI) teams. The QI teams received training on the interactive Quality Improvement Platform for Providers (QIPP) and were responsible for guiding the facilities on downloading the quality-of-care standard operating procedures (SOPs) from the QIPP, customising the SOPs for specific facility use, implementing priority activities reflected in the QIPP, and reporting on all QI activities implemented, including picture evidence, into the SafeCare platform.
The SMGL 2.0 team provided quarterly on-site supervision and virtual mentoring to the 25 facilities, and feedback was used to further improve the quality of care provided by each facility. During the quarterly supportive supervision visits, the SMGL team addressed challenges faced by the QI teams or facility staff in implementing the SafeCare model. Recommendations were made, and the implementation was tracked during subsequent visits.
Image credit: Nigeria Health Watch
In the project’s second year, a second assessment was conducted. Results from the assessment showed that 12 facilities moved up to a higher quality level (e.g., from level 1 to level 2 or from level 2 to level 3), seven (7) facilities moved up two levels, i.e., from level 1 to level 3, while five (5) remained on the same level. It appears that the act of baselining and measuring quality of care is a motivator to improve.
SafeCare for maternal health The SafeCare methodology also equipped health care providers in supported facilities with skills, tools and resources to provide quality care to pregnant mothers.
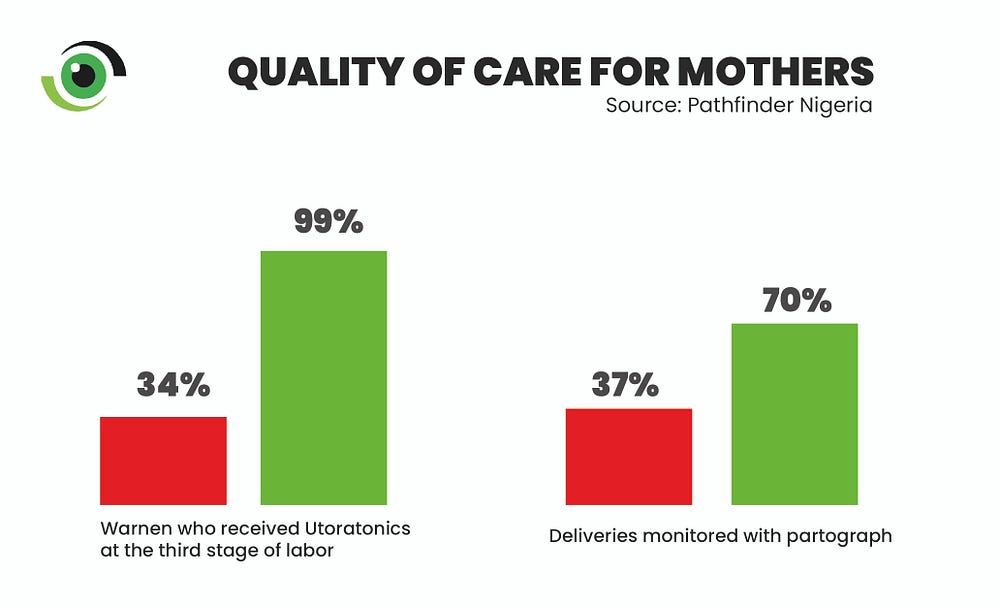
A health care worker at a hospital in Giwa, Kaduna shared how the training she received built her capacity to provide quality maternal health services to pregnant women. “We had the knowledge of all these things, but you know, after the exposure we had at the training, it was as if we never knew anything. We now have more effective solutions to better manage excessive postpartum bleeding through the active management of the third stage of labour…through the training, we have been equipped to promptly detect complications in labour and depict it in a partograph,” she said.
We now have more effective solutions to better manage excessive postpartum bleeding through the active management of the third stage of labour Photo credit: Nigeria Health Watch
The health worker passed her learnings from the training on to other facility staff and noted that everyone is working as a team to ensure positive maternal outcomes “ all of us are able to detect or identify when we see the partograph is not in order, …and we always act faster now with the use of partograph,” she added.
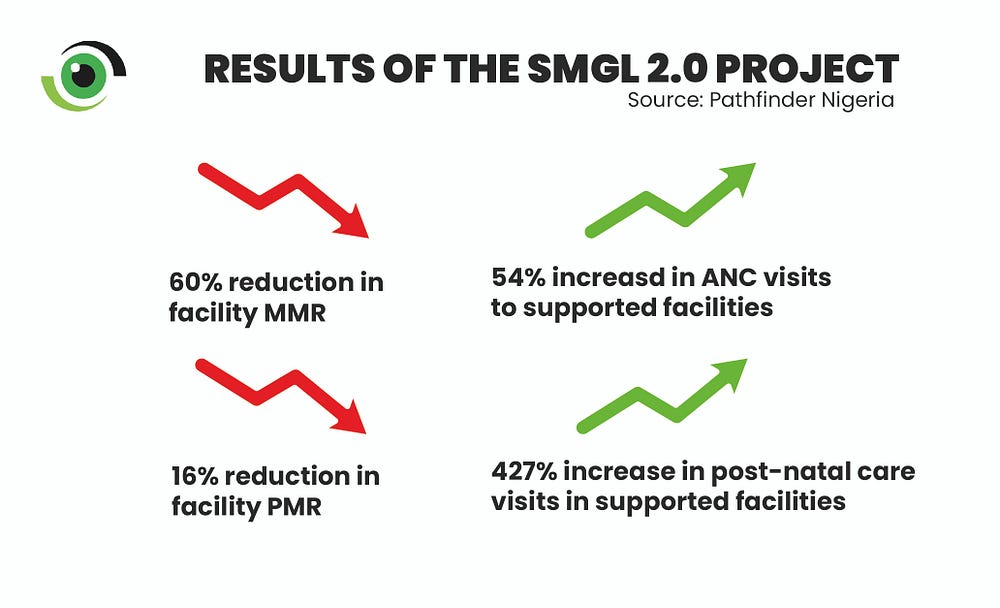
Results from the end-of-project assessment attest to the quality improvement efforts, showing that maternal and perinatal deaths in all 25 private health facilities decreased by 60% and 16%, respectively, while the percentage of newborns with birth asphyxia that were successfully resuscitated increased by 36%.
Image credit: Nigeria Health Watch
Partograph-monitored deliveries increased by 33% and births in supported facilities increased by 17%. There was a 52% reduction in stock-outs of essential medicines while there was a 65% increase in women who received active management of the third stage of labour.
Not without a few hitches One key programmatic challenge was the high attrition rate of health care providers in the private facilities. Out of the 438 health care providers who were trained, 93 (21%) resigned their services to take up new opportunities. To mitigate this, the project ensured that key staff, such as the hospital’s owners and managers, were trained, and the training was stepped down to other staff within the facilities.
Additionally, building collaboration and partnership between the facilities and the Kaduna state government initially came with some level of suspicion from the private sector. This was addressed by engaging in continuous advocacy between the government and the private health sector. According to Paulina Akanet, State Program Manager, SMGL 2.0 project, Pathfinder Nigeria, the project involved private sector associations including the Association of Nigerian Private Medicare Practitioners (ANPMP) and Association of General & Private Medical Practitioners (AGPNP), in technical working group meetings within the state to ensure inclusivity and informed discussions.
Why focus on quality care Quality care is critical to improved outcomes for maternal and newborn health. The adoption of a quality framework such as the SafeCare methodology under the SMGL 2.0 project in Kaduna state provides clear evidence that quality of care and maternal health outcomes can be improved if the capacity of private health facilities is strengthened using a quality improvement model. Scale-up and replication of this model to more private and public health facilities in more states across Nigeria would bring us closer to attaining the SDG 3.1 global target of having less than 70 maternal deaths per 100,000 live births.
This program is supported by funding from MSD, through MSD for Mothers, the company’s global initiative to help create a world where no woman has to die while giving life. MSD for Mothers is an initiative of Merck & Co., Inc., Rahway, NJ, U.S.A
Nigeria has become the first country in Africa’s “meningitis belt” to roll out a new meningitis vaccine called Men5CV or ‘MenFive’. It is the world’s first vaccine to provide protection against all five strains of the meningococcal bacteria that cause meningitis.
Around half of meningitis cases and deaths occur in children under 5 years old, according to the World Health Organization (WHO).
Since 2010, Africa, which sees the highest burden of meningitis infection in the world, has been fighting outbreaks using the MenAfriVac vaccine. Although it has successfully eradicated about 80% of meningitis infections across the continent, the vaccine only protects against a single strain of the meningococcal bacteria, serogroup A.
That means Africans haven’t had protection against the four other strains of the bacteria (C, W, Y and X), all of which cause the disease. Cases of meningitis have continued to rise in meningitis-prone areas, and have been attributed to the C, W, Y, and X strains, but not the A strain.
Last year, reported meningitis cases jumped 50% across Africa, according to the WHO.
“According to any standards, it’s unbearable to keep this disease burden,” Marie-Pierre Preziosi, an expert on meningitis at the WHO, told DW.
Between October 2023 and mid-March of this year, Nigeria experienced an outbreak of the C strain, which led to around 1,700 suspected meningitis cases and some 150 deaths across the country, the WHO reports. The vaccine was rolled out to address that epidemic.
Other countries, such as Togo, have seen similar outbreaks in past years.
Meningitis belt
Africans located in the 26 countries considered part of the continent’s meningitis belt are more susceptible than anyone in the world to meningitis. Preziosi said that is because of the area’s climate.
At any given time, around 10% of the global population is carrying the bacteria that causes meningitis in the back of their throat or nose. The bacteria normally sits in their mucus membranes, which protect them from bacterial infection spreading. Trouble only comes if that membrane is breached, allowing the bacteria to enter the bloodstream.
Preziosi said that in the dry season in Africa’s “meningitis belt”, which generally takes place between December and June, dry, dusty winds blow from east to west. When inhaled, the material that blows with these winds can breach the mucus membranes. Many studies have shown that meningitis outbreaks can be clearly tracked with this dry season.
Before the rollout of the MenAfriVac shot, countries in the belt saw major outbreaks every five to 12 years, according to Gavi, the Vaccine Alliance, an international health organization that will help distribute the shot. During the worst of these outbreaks, up to one in 100 people were infected.
Africa’s 1996-97 meningitis outbreak represents one of the country’s worst, leading to at least 25,000 deaths and infecting some 250,000.
The dusty, dry season is associated with meningitis outbreaks in sub-Saharan AfricaImage: Joerg Boethling/imago images
Meningitis causes serious long-term health issues
Even with early diagnosis and antibiotics, meningitis is deadly in about 10% of cases, and about 20% experience long-term health issues.
“For those who survive, one in five can develop long lasting disabilities — that can be neurological disabilities, loss of hearing, deafness, also losing limbs,” said Preziosi. “So it’s quite dramatic, and it can drive a whole community into poverty.”
Meningitis is most commonly spread through droplets from coughing, sneezing or kissing. The incubation period is generally between three and four days.
Initial symptoms are usually non-specific and can look like the flu. If untreated, the carrier can develop high fever, light sensitivity, neck stiffness, bleeding in the skin and, in the worst cases, blood poisoning that can lead to sepsis. Infection leads to the inflammation of membranes surrounding and protecting the brain and spinal cord.
By protecting people from all five strains of meningitis, experts hope the new Men5CV vaccine will prevent the burden of the disease initially in the African meningitis belt, but eventually in other meningitis-prone regions.
Children are the most vulnerable to life-threatening meningitis infectionsImage: ISSOUF SANOGO/AFP
Men5CV vaccine rollout
The Men5CV vaccine rolled out in Nigeria has been in the works for 13 years. It uses the same mechanism used by the MenAfriVac to fight infection.
“When you get the vaccine … your body will react in creating antibodies, these are the defense mechanisms to protect from infectious diseases,” said Preziosi. “Those antibodies could also generate some specific mucus antibodies at the surface of your nose or throat,” she said, which prevent the bacteria from latching on.
At this point, the new Men5CV vaccine will only be used to address outbreaks. The WHO hopes to see countries start launching it by 2025 for preventative measures in all children from the age of 2.
At $3 (€2.80) per shot, this vaccine is slightly more expensive than the MedAfriVac, which is less than $1 (€0.94). But Preziosi says that if there is broad uptake, the price could go down.
Preziosi hopes the new five-strain vaccine will be as successful eradicating all strains of meningitis as the A vaccine, which has almost eradicated that specific form of meningitis from the meningitis belt.
Despite having the largest economy in Africa, Nigeria also loses more women to death in childbirth than most other countries in the world. In 2020, about 82,000 Nigerian women died due to pregnancy-related complications, a slight improvement on the previous year, but an increase on previous decades.
The causes of death included severe haemorrhage, high blood pressure (pre-eclampsia and eclampsia), unsafe abortion and obstructed labour. Doctors and activists say high maternal mortality rates reflect a lack of trust in a broken public healthcare system and little political will to fix it.
The World Health Organization recommendation for a functioning healthcare system is one doctor for every 600 people; in Nigeria, the ratio is one for every 4,000-5,000 patients. The federal budget for healthcare in 2024 is 5% , a record high, but far short of the 15% suggested by the UN.
Most Nigerians live in areas without well-equipped medical centres or have to pay upfront for treatment. During pregnancy, women skip prenatal check-ups, choose traditional healers and often don’t resort to seeking professional medical help until it is too late. Nigeria’s rate of 1,047 deaths per 100,000 births in 2020 is the third-highest maternal mortality in Africa and far from the UN goal of 70 deaths per 100,000 to be reached globally by 2030.
The patient
Lawal Arinola, 31, arrived at the Lagos Island maternity hospital early in the morning. Her uterus was not contracting after a caesarean section at a private health centre the previous day. She was losing blood and had acute renal failure. The hospital lifts had been broken for months and ground-floor theatres were unavailable, so as she went into cardiac arrest she was carried on a stretcher to a second-floor operating room. An anaesthesiologist started heart massage, shouting for adrenaline to be delivered as the machine monitoring Arinola’s heart bleeped out a flat line.
It was five minutes before she was resuscitated and Dr Olusola Togunde and his team could perform an emergency hysterectomy. The room was hot and several times a nurse wiped sweat from Togunde’s forehead. He was checking for remaining sources of bleeding when the lights went out for the third time that day. In theory, every theatre in the hospital has a constant supply of energy from a generator, but this time the connection failed. The machines monitoring Arinola’s vital signs fell silent and the lights went off. Togunde made the post-operative stitches using the torch from a phone held by one of his assistants.
Despite all efforts of hospital staff, Arinola did not wake up from the surgery. The septic shock that she arrived with turned into multiple organ disfunction. She died in the hospital’s ICU eight days later.
The doctors
“The road to maternal mortality is filled with delays,” says Togunde, obstetrician and gynaecologist, and the head resident of the Lagos Island maternity hospital. In his 17 years of working he has seen tragedy after tragedy. He describes women being brought to the hospital unconscious after waiting for hours or even days before seeking medical help, because they fear the costs, or have to wait for husbands or male family members to take action.
Accessing healthcare is a problem around the country. In densely populated Lagos, with its unreliable public transport, even ambulance sirens don’t make the heavy traffic move.
There are delays too in the hospital itself. Togunde deals with patients shifted from one facility to another due to lack of space. The Lagos Island hospital has rigorous protocols. It has reduced the number of maternal deaths in the past 10 years from 93 in 2013 to 38 in 2023.
Where an emergency caesarean is required, the patient has to reach surgery within 30 minutes. Posters outlining the hospital rules and its efforts to fight maternal mortality adorn the walls of the hospital. Medicines are kept ready in the emergency room, so relatives do not need to go to a pharmacy to buy them, as often happens in other hospitals; and there is an emergency fund for the poorest, paid for by donors and sometimes doctors too. Yet, still the hospital struggles.
The dire state of healthcare prompts many medical professionals to emigrate, exacerbating the problems.
“Manpower is a problem,” says Togunde. “We have space, but sometimes we don’t have people to operate. The hospital does not employ staff [they are employed by the government], it is beyond our competence, and doctors emigrate. The young ones don’t even stay. Sometimes people just leave without notice, so you cannot guarantee the number of staff you will have the next day.”
“I understand that people are dying from lethal diseases, but pregnancy is not a disease,” says Dr Moses Olusanjo, a senior consultant at the maternity ward of Lagos State University teaching hospital, the principal referral centre for patients in Lagos with complications. Olusanjo has worked there and at Lagos Island hospital for more than 11 years, but is now planning to continue his education – and possibly his career – abroad.
“When you go to countries like the UK, women don’t die like here,” he says. “The problem of maternal mortality is a reflection of how our society works. Until the standard of life increases, this will not go away. The reduction of maternal mortality is solely within the power of our leaders. The problem is too vast for doctors alone to handle. It takes political will to say that our women will not die.”
The activist
Abiola Akiyode-Afolabi runs the Women Advocates Research and Documentation Center (WardC), an organisation aimed at combatting maternal mortality and gender-based violence. She had two very different experiences giving birth to her own children, one in the US and one having an emergency caesarean in a public hospital in Lagos.
“After the surgery in Lagos, I was left on a bed in a corridor while I was still bleeding,” she says. “For two hours, I was screaming for help.”
When Akiyode was finally taken by her brother to a post-delivery room, she was forced to switch beds and bathe alone just hours after the surgery. There were no sanitary products. Some of the women she shared a ward with were taken for emergencies at night, and never returned.
“I believe that they died,” she says. “This was the first time that I realised how often women were dying in this country. I saw it firsthand. It was like a mortality centre, this ward called Ward C.” Later, she named her organisation after the place of her traumatic experience.
Akiyode believes much greater political commitment is required. In 2014, her organisation and several others filed a petition to the African Commission on Human and Peoples’ Rights, charged with ensuring that African states comply with human rights obligations, to reaffirm Nigeria’s duty to end preventable maternal mortality. “We hope it will help to increase budgets, establish a national plan and take the matter seriously on a national scale,” she says.
The survivor
In the post-delivery unit of Lagos State University teaching hospital, Torkwase Umoru, 26, was discharged in time for her daughter’s first birthday. A month earlier, she started having abdominal pains and went for a scan at a private hospital in Lagos where she learned she was pregnant and that the foetus had died.
She underwent an evacuation, but over the next few days the pain became unbearable. By the time she was brought to the emergency unit, she had sepsis, a perforated bowel, and her life was in danger.
Torkwase Umoru shows her scar. ‘After all I went through, I don’t think that I want more kids,’ she says
Umoru is still not sure what lead to the development of such a severe condition, whether it was uterine fibroids already present before the first pregnancy, or the way her stomach was sewn after an emergency caesarean when her daughter was born; was it a poorly performed evacuation of the dead foetus days earlier, or a lack of a proper diagnosis?
Even after surgery she did not feel better. She could not eat or drink, a colostomy bag had been attached to the side of her stomach and was burning her skin. Her husband stopped going to work and visited her every day to clean her wound.
“I felt depressed, ashamed, worthless,” she says. “But I was not afraid of dying. In fact, at that point I wanted to die. My husband told me later that he was hiding all sharp objects from my sight. He knew that I could try to hurt myself, that I was thinking about that.
“Now, after all I went through, I don’t think that I want more kids. We will maybe try to adopt,” she adds.
The foster mother
In a chemist shop in rural Ota on Lagos’ outskirts, Damilola Ayomide, an auxiliary nurse and mother of three, sells basic medicines such as painkillers, as well as children’s clothes and bread. Otherwise, the shelves in her store are almost empty.
She keeps an eye on the baby asleep in a basket on the ground. It is her younger brother’s son, Oluwaremilekun, which means “God wipe my tears” in Yoruba.
His mother, Seun Fadipe, 27, died three days after his birth at a local hospital. During pregnancy she was often sick, her legs were swollen and she fainted several times. Ayomide says the family would take her to a hospital each time, but she was always discharged within a few hours after being put on a drip and medication.
When the time came, Fadipe was so weak that the family raised money for a caesarean section. It went well, they were told, and Ayomide visited her in a hospital the day before she died.
“The hospital just called my brother to tell him that his wife was dead,” says Ayomide. “We don’t have any documents; we don’t know what exactly happened. They said that she was complaining of a headache and abdominal pain, but died before the nurses came to check.
“We could not believe it. It was so painful for my brother, I’ve never seen him like that. We all cried so much, but what could be done? It was God’s will to take her.”
Afterwards, the family decided it was best for Ayomide, with her nursing experience, to look after the baby. “I now go everywhere with the baby. I put him in a chair or in a bed and attend to my patients. Sometimes, I have to stop the visit if he cries. Last time, when I left him with a friend for a few days, he got a fever. He does not like being anywhere else. I’m his mama now. But it affects me a lot, I have my own children to take care of,” she says.
In Nigeria people depend on their extended families, especially the women who hold communities together. Every time Togunde loses a patient, he wonders about her family. He sees the pain of her parents or partner but thinks of the consequences that go further.
“Each time with a death of a mother, a household, a community, is destroyed,” he says. “The children she had don’t have their primary carer – some drop out of school, most are sent to distant relatives; siblings are separated. Once the mother is gone, her family is scattered. Their home no longer exists.”
Drug regulators in Tanzania, Rwanda and Zimbabwe have recalled a batch of Johnson & Johnson children’s cough syrup as a precautionary measure after their Nigerian counterpart said laboratory tests found high levels of toxicity.
The countries join Nigeria, Kenya and South Africa in recalling the same batch of the syrup, which is used to treat coughs, hay fever and other allergic reactions in children. South Africa has also recalled an additional batch.
Laboratory tests on the syrup by Nigeria’s health regulator showed a high level of diethylene glycol, which has been linked to the deaths of dozens of children in Gambia, Uzbekistan and Cameroon since 2022 in one of the world’s worst waves of poisoning from oral medication.
Diethylene glycol is toxic to humans when consumed and can result in acute kidney failure.
The batch of Benylin Paediatric syrup recalled was made by J&J in South Africa in May 2021, although Kenvue now owns the brand after a spin-off from J&J last year.
Tanzania Medicines and Medical Devices Authority (TMDA) said it had begun the recall on April 12 after hearing about the Nigerian test results.
“This is an exercise that does not involve investigation but rather monitoring to ensure that those affected drugs are removed from the market,” TMDA spokesperson Gaudensia Simwanza told Reuters on Monday.
A spokesperson for Kenya’s drug regulator said its test results on the syrup would likely be ready on Wednesday.
“A review of our safety database doesn’t reveal any adverse events reported,” the Rwanda Food and Drugs Authority said in a statement dated April 12. “However, Rwanda FDA issues the present recall for precautionary measures.”
Zimbabwe’s Medicines Control Agency said that it did not have a record of the product’s importation into Zimbabwe, but that it was concerned the syrup could enter the local market illegally. It said it would step up inspections in case.
A leading Afro-focused multinational company, Shalina Healthcare has reiterated its commitment to delivery of quality healthcare in Nigeria and other African countries.
The Chief Commercial Officer, West Africa of the company, Arun Raj, declared this in Lagos on Monday, at the closing of its 2023/24 financial year and celebrate its 40 years of its existence.
“The company is determined to continually fulfill its corporate mission of making quality products available to every African at affordable prices.
“It has been 40 years of trust in Africa and these 40 years, the people of the continent have also reciprocated the trust in our quality products and healthcare delivery.”
In his corporate presentation and new financial year projection, the Head, Corporate Marketing of the Company, Folorunso Alaran, said ”it is building on the trust Africans have in its products and services over the year and is committed to healthy Africa.
“It has been 40 years of available, affordable and quality products for Africans.”
Mr Nirmal Jain, CEO Shalina consumer Global, said, “we believe that every African must have access to good products.
“And, for the last 40 years, we have been trusted for our quality products and more so, through our many initiatives and healthcare interventions, Shalina has continually raised the bar in healthcare delivery.”
Speaking further, Mr Debajeet Mukherjee, CEO Shalina Pharma Global, posited that; ” in spite of the prevailing economic challenges, we do not waver in delivering our corporate purposes of available, affordable and quality health products.
“It is our belief that economic challenges should not hinder people’s access to quality healthcare. Either the economy is good or bad, it shouldn’t affect the lives of the people in an adverse way.
“In spite of the fact that some companies are leaving Nigeria, we are expanding our team in the country. This is because we have trust and believe in Nigeria.”
In her own presentation, the Company’s Managing Director, Nigeria, Opeyemi Akinyele, said ”the company is focused to become number one brand in Nigeria and continually promote the best of healthcare delivery in the country.
“Through our products, activities and interventions, we have been doing greatly to ensure that quality healthcare is available and affordable for every citizen. And this is a promise that will remain unbroken,” she said.
She appreciated members of staff of the company for their commitment and supporting roles in the company, saying that, “without you, your roles and efforts, we won’t be here and the successes recorded in the out gone year won’t be possible.
“We also rely on your continuous support and commitment in the new year.”
The high point of the company’s end of year activities, include honouring some members of staff members with awards of excellence in different categories for 2023/24 financial year.
Amongst them were: Lasisi Abiodun, Best Pharma Delegate, Lawal Abubakar, Best Medical Delegate, Ruth Adewoye, Best Regional Manager Pharma, Ganiyu Lateef, Best CVD Delegate, Mercy Omoji, Best Regional Manager and Consumer,
Others are: Uzuma Pascal, Best Zonal Manager, (Global) and Juliet Edward, Best Consumer Delegate Global, while winners in other categories included Sandeep Sahu, Folorunso Alaran, Emeka Adimoha, Chiuba Nwaosu, among others.
Shalina Healthcare which began its business in Africa in DR Congo in 1984 made entry to Nigeria 25years ago and currently has about 2500 staffs globally out of whom 2000 are in Africa. (NAN)